This week, when I was researching some sources on late seventeenth-century iatrochemistry, I ran across a reference to the work of Philip Verheyen (1648-1710), a farmhand-turned-anatomist. I had never heard of him before, but thought his work might be interesting for me, so I did what every person, including an academic, does these days: I googled him. And clicked the first link: a Wikipedia page. A bit surprised that a quite detailed Wikipedia page in English, complete with painted portrait was dedicated to a relatively obscure seventeenth-century Flemish anatomist, I started reading. It all seemed genuine enough, with references to the work of known Dutch historians of medicine such as Lindeboom. Until I read that Verheyen had dissected his own leg and suffered phantom pains after it was amputated, and that this
‘…prompted him to take up a career in anatomy in order to probe and understand this phenomenon and also write the deeply personal series of notes (1700-1710) that may be translated either as “Notes on My Amputated Leg,” or “Letters to My Amputated Leg,” the former seeming more probable, while the latter is more in keeping with the tone of the notes.’
Verheyens 1693 ‘Corporis Humani Anatomia’ was reprinted 21 times and translated in several languages.
I bet you clicked the link to the Letters, didn’t you? I did! And it’s a stub. Some people may now think ‘well, duh, of course, you shouldn’t just believe everything that’s on Wikipedia.’ Obviously you shouldn’t (as I keep stressing when I’m lecturing too), but by now I have read so many weird and wonderful things about early modern medicine and chemistry that a small part of me still wondered whether there was some truth to this story. So I looked Verheyen up in Picarta (the Dutch national library catalogue, a sort of Worldcat). He did indeed exist, wrote quite some interesting things on anatomy, but no letters to his leg. The other references I could check online do mention the amputated leg, but no dissection or letters.
Then I continued reading the Wikipedia page and noticed that the author says that Verheyen studied at the Leids Universitair Medisch Centrum – indeed an existing institution, but a profoundly twentieth-century institution. A bit annoyed with this nonsense now, I scrolled back up and had a closer look at the ‘painting’ of Verheyen dissecting his own leg. Now I immediately saw it was not a painting at all, but a digitally composed image – I actually recognized ‘Verheyen’ as one of the onlookers in Tulp’s Anatomical lesson. When I magnified the image, I noticed the bare ‘stump’ of the leg under the table, and couldn’t help laughing. Someone had put a lot of thought into this!

Rembrandt, The Anatomy Lesson of Dr. Nicolaes Tulp , 1632. Oil on canvas. Mauritshuis, The Hague.
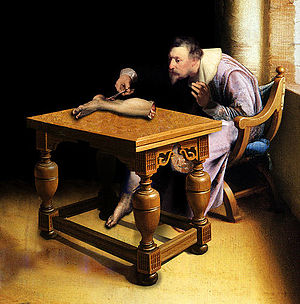
Philip Verheyen Dissecting His Amputated Leg. According to Wikipedia: “Anonymous. From the collection of Pieter Deheijde.”
Back to Google, I found that the sixth hit was a link to a project of a New York-based artist, Sreshta Rit Premnath. It turns out that the ‘painting’ and the entire Wikipedia page on Verheyen are part of an art project. In a response to a message written by someone who did not notice the inconsistencies, Premnath readily admits that the Wiki is largely fictitious, and the portrait a digital creation. Yet it is not some silly joke; Premnath raises some serious questions with this project. As he puts it himself:
‘Do we not all perceive the world through images that are given to us through books and media; and through the socio-political contexts in which we are brought up? The painting “Philip Verheyen Dissecting His Own Amputated Leg” does not actually exist. It is a composite image I have created in order to explore this fragility of truth and authenticity.’
I think the way Premnath has chosen to raise these questions is quite brilliant, as even people who are generally considered to be relatively smart and critical-minded (historians like myself, the author of the message Premnath is responding to – who is apparently a medical doctor) are initially willing to believe that Verheyen really dissected his own leg and wrote letters to it. This may seem silly, but on the other hand open-mindedness is also required to be a good academic. This balancing of open-mindedness and critical thinking also reminded me of another exploration of the fragility of truth and authenticity I really love: David Wilson’s Museum of Jurassic Technology in Los Angeles. This museum leaves visitors wondering which of its exhibits are real – yet they are all wonderful. I had the pleasure of visiting the museum in 2010, but if you can’t, do read Lawrence Weschler’s Mr. Wilson’s Cabinet of Wonder. Pronged Ants, Horned Humans, Mice on Toast, and Other Marvels of Jurassic Technology.
Although I admit I was a little annoyed when I initially discovered I was being ‘fooled’ with the Verheyen Wiki, I think projects like Premnath’s and Wilson’s are more than necessary to keep everyone, including, or maybe especially us academics, sharp and critical about what we understand as true and authentic and factual. Contemporary art can hold up a mirror, and show us how we often construct stories unthinkingly – and that it is the task of the historian to undo these constructions and think them through and reconstruct them into histories. Only to humbly realize that those histories are also stories, of course.










You must be logged in to post a comment.